17. EtOH Disinhibition & CSubs Abuse - RonaldMah
Ronald Mah, M.A., Ph.D.
Licensed Marriage & Family Therapist,
Consultant/Trainer/Author
Main menu:
17. EtOH Disinhibition & CSubs Abuse
Therapist Resources > Therapy Books > How Dangerous
How Dangerous is this Person? Assessing Danger & Violence Potential Before Tragedy Strikes
Chapter 17: EtOH DISINHIBITION & CRANKSTERS PLUS- SUBSTANCE ABUSE
by Ronald Mah

Chapter 17: EtOH DISINHIBITION & CRANKSTERS PLUS- SUBSTANCE ABUSE
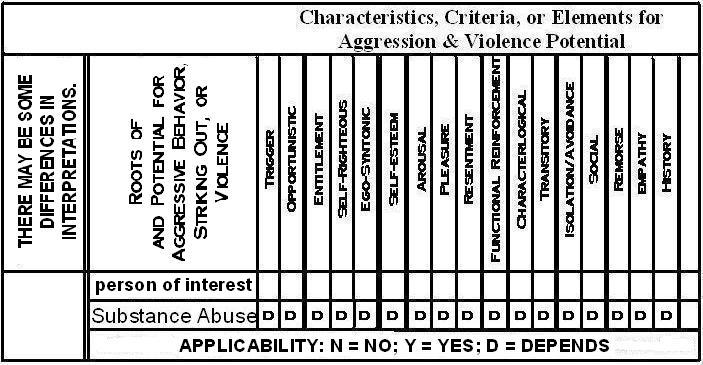
SUBSTANCE ABUSE: Characteristics, Criteria, or Elements for Aggression & Violence Potential
-- Code: NO=not applicable; YES=applicable; DEPENDS= Depends on other issues or occurs sometimes
SUBSTANCE ABUSE: DEPENDS, Specific Triggering EventSUBSTANCE ABUSE: DEPENDS, Opportunistic BehaviorSUBSTANCE ABUSE: DEPENDS, Sense of EntitlementSUBSTANCE ABUSE: DEPENDS, Self-Righteous AttitudeSUBSTANCE ABUSE: DEPENDS, Ego-syntonic PerceptionSUBSTANCE ABUSE: DEPENDS, Self-Esteem Gain or LossSUBSTANCE ABUSE: DEPENDS, Intense Emotional ArousalSUBSTANCE ABUSE: DEPENDS, PleasureSUBSTANCE ABUSE: DEPENDS, ResentmentSUBSTANCE ABUSE: DEPENDS, Functional Reinforcement (positive or negative)SUBSTANCE ABUSE: DEPENDS, Characterlogical Behavior/PerceptionsSUBSTANCE ABUSE: DEPENDS, Transitory Behavior/PerceptionsSUBSTANCE ABUSE: DEPENDS, Isolation/Avoidance BehaviorSUBSTANCE ABUSE: DEPENDS, SocialSUBSTANCE ABUSE: DEPENDS, Presence of RemorseSUBSTANCE ABUSE: DEPENDS, EmpathySUBSTANCE ABUSE: DEPENDS, History
Owen, who was discussed with respect to paranoid personality disorder drank alcohol and used crank- methampethamine abusively. Alcohol abuse or use is often correlated to domestic violence and other types of violence or abuse. Other substance abuse or use comprised of various illicit and legal drugs or medications may also have association with violence. It is apparent although not always clear to what degree alcohol or drugs cause or contribute to violence. “Over time alcohol and drugs have been linked to anger and aggression. Alcohol, stimulants (cocaine and methampethamine), anabolic steroids, marijuana and other drugs have either been used to ameliorate uncomfortable emotional states or have been implicated in the precipitation of anger and aggression. Not only do many of the mood altering substances impair perception but also there is proof that alcohol and drugs -- through their ability to alter neurotransmitter levels alter mood state” (Dual Diagnosis Recovery Network, 2012).
As with the potential for violence with psychotic individuals, with substance abuse affecting violence potential, it depends. By definition use becomes abuse when there are problems associated with use. Problems in physical or medical health, psychology or emotional well being, relationships, and academic or vocational functioning are the key criteria where harm can result from abuse of substances or continued behaviors. Abuse is considered addiction when inability to refrain from use, craving, repeated failed attempts to stop or cut back, obsessive and compulsive financial or energy (including mental) dedicated to acquiring, use, and hiding use, and increased tolerance causing greater indulgence to gain effects become associated with the identified problems. Emotional volatility including anger resulting in aggression and violence with others including partners can be the result of or correlated with substance abuse or addiction. Alcoholism, drug abuse and addiction, and behavioral addictions can become destructive and a focus of treatment or intervention for an individual, in a couple, at school or work, and in the community at large. For this discussion, their relevance to violence potential is considered.
The degree of violence potential depends on the individual’s personality, the nature of the effect of the substance, and the interaction between personality and the substance. Methampethamine or crank, cocaine, crack, and other stimulant drug abuse can cause paranoia and tend to mimic paranoid personality disorder. “The leading causes of death for cocaine and methampethamine addicts are violence, suicide and accident. All are violent and also may have strong connections to toxic alterations of the neurotransmitters norepinephrine and dopamine. During toxic episodes stimulant drugs can create an elevation of both norepinephrine and dopamine. Increased norepinephrine levels create a state of hyperarousal. This is similar to the ‘fight or flight’ response that manifests during times of real or perceived danger. Combine this with continued elevations of dopamine and there is a potential for a paranoid state. As dopamine starts to elevate in the brain, the user experiences context appropriate paranoia. A good example of this is the sense that every sound outside of your apartment is a narcotics agent causing the individual to constantly look thru the peephole in the door. As dopamine levels continue to elevate with continued use of a stimulant drug a presentation develops that looks like delusional (paranoid) disorder. Persecutory, jealous and other delusions can exist. A man in a treatment program once described a paranoid delusion that occurred in the early morning hours after a night of heavy free base usage. He believed that there were unmarked police cars parked up and down his street. In order to check and see if they were there, he would walk out of his house every fifteen minutes to look inside his mailbox while scanning the street for unmarked police cars. He felt that this was the only inconspicuous way he could check for signs of trouble” (Dual Diagnosis Recovery Network, 2012). To a methampethamine abuser- the "crankster," the police as the object of paranoia can be easily substituted with the partner, family member, acquaintance or friend, neighbor, or colleague or boss. Scrutinizing for “signs of trouble” from this paranoid place predicts violent actions. A stimulant drug user or abuser may have a profile of the seventeen characteristics essentially identical to the individual with paranoid personality disorder.
“‘Stacking’ and ‘pyramiding’ anabolic steroids can create symptoms from rage to psychosis. ‘Stacking’ means that more than one anabolic steroid is being used at the same time. For example, an injectable can be added on top of oral ingestion. ‘Pyramiding’ refers to the escalation of dose of the steroids. As the dose levels increase, rage and aggression may be a symptom of the drug experience” (Dual Diagnosis Recovery Network, 2012). Steroids are an example of a medication or drug that is not always seen as prompting or releasing anger and aggression. However, in certain situations and in combination with other altering substances and psychosocial circumstances, unanticipated intense feelings may be triggered. Marijuana is not anticipated to be an enraging or aggression inducing substance for example. “‘Let’s get mellow’ and ‘let’s chill out’ are subjective terms used to describe the cannabis experience. These phrases seem to indicate a desired experience secondary to inhalation. It appears that many marijuana users are using the drug to reduce levels of anger and/or anxiety. Clinicians should look for these emotional expressions in the patient and if they do not disappear quickly (remember the abstinence syndrome can manifest as anxiety and irritability lasting for up to three days after cessation and these symptoms can come back in an exaggerated fashion in 3-6 weeks) they should be treated as an underlying problem and a relapse issue” (Dual Diagnosis Recovery Network, 2012). However, sometimes marijuana use can cause fear, anxiety, panic or paranoia, which may prompt aggression. Violence is more prevalent among habitual marijuana users versus occasional users. The reason for this is not clear. It “may be because people with violent tendencies can also have a range of other psychosocial problems and are therefore more likely to use marijuana” (National Cannabis Prevention and Information Centre, 2012). Since marijuana is illegal, involvement in the drug market trade may increase the chance of violence. “Research also shows that marijuana users who commit violent acts usually have a history of violence before they start using the drug.” Withdrawal often is accompanied by irritability and other symptoms, which may influence violence. There can be psychotic reactions, confusion, feeling threatened or scared, and paranoia that result in aggression and violence as well. As a result, some users may have profiles of the seventeen characteristics once again essentially identical to the individual with paranoid personality disorder. There may be similar dynamics with other substances leading to aggression and violence not commonly associated with recreational use.
Alcohol is a socially accepted mind and mood altering substance for recreational use. Gaia is a very relaxed drunk. Sam is a happy drunk. Olivia is a silly drunk. Stephanie is a melancholy drunk. Brit however, becomes mean when intoxicated. Michel is an angry, aggressive, and violent drunk. Johnny becomes paranoid. Bernie is more arrogant- basically, narcissistic. Kennedy becomes hypersensitive to betrayal, abandonment, and rejection- fairly borderline. Jul gets very needy- dependent. Sharon becomes very demonstrative and flamboyant- histrionic behavior. The varied effects of alcohol have to do with its effect on the inhibitory function of the brain. “The notion that alcohol intoxication impairs behavioral inhibition, and, by extension, facilitates aggressive behavior, is well engrained in both the scientific literature and popular culture. Impaired inhibitory control, also referred to as disinhibition, can be described as a lack of cognitive and/or behavioral restraint that can result in a number of maladaptive behaviors” (Giancola et al., 2010, page 265). “Although the association between alcohol intoxication and behavioral disinhibition seems obvious, so too is the fact that alcohol does not cause inappropriate dyscontrolled behavior in all people. We are all aware of alcohol’s ‘Jekyll and Hyde’ effect in which people who are typically well tempered when sober sometimes transform into violent barbarians when intoxicated. Alternatively, we are also aware of people who simply become more talkative, friendly, and flirtations when equally intoxicated. (Giancola et al., 2010, page 266). Since there are so many potential responses to alcohol, it has been speculated that alcohol releases aggression only for individuals already predisposed to aggression.
The individual may have significant aggressive feelings and thoughts. He or she may have histrionic, dependent, borderline, narcissistic, paranoid, or antisocial tendencies and urges but is largely successful in inhibiting them. Or, had lashed out in frustration or bullied previously and suffered negative reinforcement and now refrains from being aggressive. Prior cultural validation and modeling of aggression may have come up against social sanctions and/or a cross-cultural model intolerant of aggression. Aggressive or violent feelings or thoughts under active inhibition do not express overtly victimizing another person. Alcohol use otherwise benign in others becomes alcohol abuse as in an individual whose disinhibited feelings and thoughts prompt or release aggression and abuse. As a result, when under the influence an individual with otherwise relatively low violence potential may have a more potentially violent profile of the seventeen characteristics similar to someone with a personality disorder. For example, when intoxicated the individual may exhibit behavior similar to someone with a borderline personality disorder. Celeste was broken-hearted when her boyfriend left for another woman. However, it was only after several rounds of margaritas at the bar did she drive to his house and smash his car windows.
Another relatively non-violent individual may be prone to narcissistic aggression, or paranoid rage and violence, or antisocial abuse when disinhibited because of alcohol use. No one may believe that Brit is narcissistic much less abusive as she moves through family, social, and work situations. However, Brit may be a hidden or well-modulated narcissist whose aggression berating her husband only comes out when she is drunk. Michel got into some intense trouble as a pre-teen and teen for animal cruelty and some particularly cruel “pranks.” His graphic and violent stories alarmed his teacher and he was brought to the attention of the school and parents. Michel figured out that he could not act out his urges without getting into worse trouble. He learned how to restrain himself and act civilly with others. Therapy helped a lot. Church and religion helped more. However, the urges never went away. They were just under his active control. Alcohol opened the valve and Michel became prone to vicious aggression and abuse of his wife and children. When sober again, Michel would suffer the punishment for his abusive actions (or alternatively, get away with it) and effectively live as a good citizen, loving husband, and caring father.
The therapist, professional, or concerned person could or should ask the individual about his or her alcohol use or drug use and how its effects, “What happens when you drink or use? How to you behave when you are slightly to highly intoxicated or high? How are you different?” Specifically, the individual should be asked, “Are you more emotional, more intense, or more aggressive when intoxicated or high? How is your judgment?” The therapist, professional, or concerned should ask the others involved or familiar with the individual for his or her experiences with the person’s drinking or use and behavior patterns. This is can be a separate but related discussion to whether there is dependence or addiction. The individual does not have to be dependent or an addict to have problems when disinhibited from alcohol consumption. These inquiries explore the differences between use and abuse- or what kind of drunk someone is. Hence, they help determine how dangerous someone may be. With substance use that becomes substance abuse, the general answer to the applicability of each of the seventeen criteria and the resultant profile is again, “It depends.” However, this apparent ambiguity can be brought to more definitive diagnosis through questioning and exploring the nature of substance use and abuse- and, the individual’s normal reaction to use.
Therapy, treatment, or an attempt to facilitate change is significantly simpler working with someone whose personality disorder tendencies expresses only when under the influence, than with someone who has an operational and functionally problematic personality disorder whether drunk or sober. In the case of profiles involving substance abuse that mimic the personality disorders, the individual may already have sufficient emotional, psychological, intellectual, and interpersonal skills to otherwise successfully inhibit inappropriate or violent behavior. Staying sober or abstinent is sufficient to preclude aggression, abuse, or violence. In comparison, getting someone with a consistently operational personality disorder to inhibit him or herself is extremely difficult. With this diagnosis, therapy or treatment would focus next on stabilizing sobriety and preventing relapse that could result in further inappropriate behavior or violence. Subsequent to or in conjunction with stabilization and relapse prevention could be addressing the underlying tendencies causing aggressive or violent feelings and thoughts. This can include how and why the individual may have been unaware of his or her tendencies and how he or she loss vigilance. The major challenge to sobriety, acting out personality disordered behavior, and reducing aggression, abuse, or violence is the likelihood that substance use and abuse is the person's primary form of self-medicating the emotional distress of the personality disorders. While therapy or treatment’s focus may shift to dealing with substance abuse as the key violence prevention strategy, the multi-layered quality of dysfunction creates inherent complications. Violence potential assessment for this type of individual is largely based initially on his or her likelihood to use substances, but must become more nuanced out of necessity.
