18. Pattern, Process, & Plan - RonaldMah
Ronald Mah, M.A., Ph.D.
Licensed Marriage & Family Therapist,
Consultant/Trainer/Author
Main menu:
18. Pattern, Process, & Plan
Therapist Resources > Therapy Books > Mine Yours Addiction- Cpl
Mine, Yours, and Ours, Addiction and Compulsivity in Couples and Couple Therapy
Chapter 18: PATTERN, PROCESS, AND PLAN

The following, A Process for Success & Growth can be used to help individuals, couples, and families uncover the process and pattern of dysfunction, identify self-sabotage and give guidance as to how to make productive change. The metaphor from Charles Dickens's, "A Christmas Carol" (1843) refer to the three ghosts that visited Ebenezer Scrooge: the ghosts of Christmas past, present, and future. The ghost of Christmas past made Scrooge nostalgic for what he had and lost, but he did not change. The ghost of Christmas present showed him the circumstances of Tiny Tim's illness and impending death that were upsetting, but he was not compelled to alter his behavior. Finally, the ghost of Christmas future took him to see his dismal fate if he continued his negative ways. It scared the heck out of him! Only then, did Scrooge find motivation to change. Awareness of his devastating future is what prompted him enough to make present day change. The therapist may need to metaphorically be the "ghost of life future." And, predict the negative fate of the individual and couple if the problematic behaviors continue. Instead of waiting for someone to hit bottom as per twelve-step principles, the therapist takes the bottom and hit the individual with it! The therapist can make vivid the consequences of the individual's continued use or behavior in the hope that it will be motivating enough for the individual to consider change.
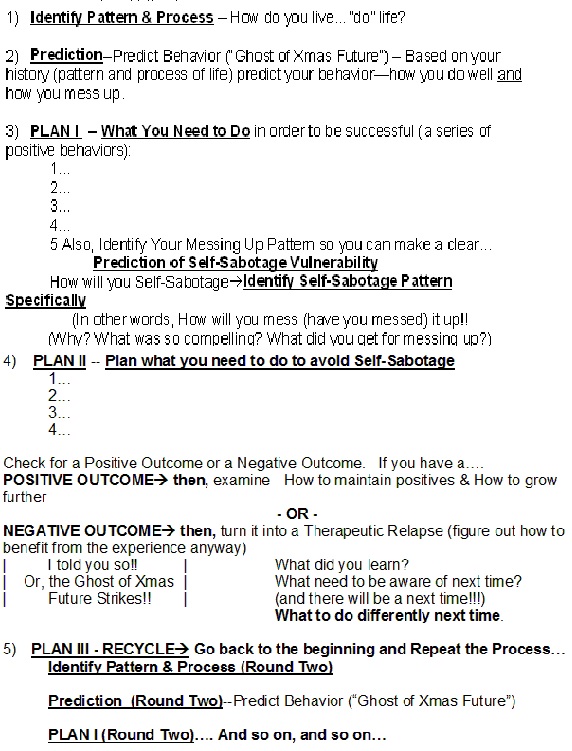
A PROCESS FOR SUCCESS & GROWTH
IDENTIFY PATTERN & PROCESS
The therapist needs to identify the individual and couple's pattern and process of dysfunctional behavior. The dysfunctional behavior may not be limited to substance abuse or compulsive self-destructive addictive behavior. This strategy for intervention can be used for any problematic pattern of behaviors. Each person and the couple tend to live their lives in some kind of pattern of choices, behavior, consequences, and reactions. To develop a process for success and growth, one often needs to first identify what the dysfunctional pattern is all about. Some people have developed a pattern and process for failure and continued disappointment. Change and growth start with identifying poor habitual choices and behaviors. In this step, the therapist needs to help the couple, as individuals and as partners identify the pattern and process of their individual life choices and their couple's relationship. The emphasis is on what happens and how it happens versus who may be right or wrong… good or bad. Positive patterns and processes should be identified, validated, accentuated, and perpetuated. However, when the pattern and process is problematic such as when it involves substance abuse or compulsive self-destructive behaviors, then they need to be minimized, reduced, or eliminated.
The addict often is already aware of his or her pattern and process. The therapist however may find that the addict has purposely, semi-consciously, or unconsciously minimized, denied, or forgotten how his or her process developed over time. Or, what the nuances of his or her pattern of use and behavior may be. The individual may offer perfunctory explanations and descriptions that are diverting and evasive. The therapist should be aware that the addict usually has a long history of deceiving both others and him or herself about use and behavior. The evasion, minimizing, deception, and lying is so embedded that he or she often is not consciously aware of them being distortions. Trusting the individual to be objectively honest and candid would be a mistake. The therapist however should explore the subjective "truth" the individual holds as essential to his or her addict "reality" and identity. The emotional and cognitive elaborations or deviations may be essential to his or her self-serving pattern. The therapist's familiarity, knowledge, and expertise about addictions will support therapeutic strategic incisiveness to identify how the common patterns and processes of other addicts may be replicated in the individual.
PREDICTION
Based on the individual's and couple's history- that is, pattern and process of life the therapist can predict individual and couple's behavior. Together they can predict how each will and the couple will do well and how they will mess up. The therapist predicts the pattern and process specific to substance use or compulsive behavior. In addition, the therapist can predict the role substance use or compulsive behavior will continue to play in the overall pattern and process in life and specifically, in their relationship. The probable or even inevitable negative experiences to come in life create motivation for change. In the "Christmas Carol" by Charles Dickens, although the Ghost of Christmas Past haunts Scrooge and the Ghost of Christmas Present makes Scrooge sad, it is the Ghost of Christmas Future that scares the heck out of Scrooge about what he is doomed to endure if he does not change his ways! The prediction of what the individual or the couple will continue to do poorly, how they will continue to fail, and how it will become more onerous and painful is what can motivate them to make the real changes in life. The therapist may need to disconnect from his or her "nice" instincts, and become somewhat brutal describing the future for the individual and couple. Rather than being gentle trying not to provoke discomfort, the therapist may want to make the vision of the individual's future as disturbing as possible. Gentle persuasion may be too circumspect to have any significant impact.
Sometimes, one or both members of the couple have already seen the dismal future. They are terrified that their vision of the couple's dismal future will become true- separation and divorce. If only one partner sees the impending apocalypse, then it becomes important to make the prediction real to the other partner. The entry into couple therapy or treatment may have derived from one or both partners sensing the impending demise of the relationship as a consequence of continued use or behaviors. The therapist should take this motivation and accentuate and amplify their concern and worry. This is often necessary since such the addict's awareness of use and behavior outcomes is transitory. As awareness and insight comes, it is also relatively sure to dissipate go when impulses and cravings reassert. The therapist may need to frequently and consistently reintroduce and remind the partners of painful future consequences. The therapist needs to be a relentless foreboding prophet especially during the "honeymoon" periods of idealistic optimism and false hope characteristic of both the user/addict and the co-dependent/enabler or co-addict.
PLAN I — WHAT YOU NEED TO DO
The therapist needs to help the individual and the partners develop a plan in order to successfully reduce and abstain from use and behaviors. The plan needs to be a series of positive behaviors. The individual once he or she finds motivation to change often only has a "try harder plan." Unfortunately, the "try harder plan" is essentially taking what has already proven not to work overtime and history, and then apply it again even more intensely in the present and future. Essentially, the addict has tried to resist craving, reduce use, and avoid being exposed. Those strategies have not worked, but the addict tries to resist harder, more deeply reduce, and hide harder. Intensification does not deal with core issues and fails to make any real enduring difference. It is critical for the individual and couple to do things differently. He or she and the couple must come up with a specific plan, probably a plan with several components or several sequential steps. A plan that is merely based on not doing negative behaviors will not normally suffice. Resisting or denying compulsive negative use or behaviors (or resisting or denying harder) does not guide the individual towards productive choices or behavior. twelve-step programs have basic recommendations to maintain sobriety or when there is craving to use or relapse (AAHistory.com, 2012). They are
Get a SponsorCall Your SponsorGo to MeetingsWork the steps in the Big Book.
Working the steps is more involved, but in the immediate period of craving, this usually translates behaviorally into three simple actions: call ones sponsor, go to a twelve-step meeting, or read the Big Book- the book of Alcoholics Anonymous. While there may be disagreement about the efficacy of the three behaviors to curtail or stop use, the three actions provide concrete active alternatives to addictive behavior. Addictive choices are interrupted when the individual either talks to his or her sponsor, attends a meeting, or reads the Big Book. The key may not be how impactful the three actions may or may not be, but that the addict is involved doing something that is not drinking or otherwise engaged in other addictive use or behavior. The therapist should help the individual and partners create a plan with specific potentially positive behaviors that are actionable. The actions are should be productive, but must definitely interrupt the pattern and process of dysfunction. Stopping negative behaviors is a given goal, but trying to stop alone is incomplete to constitute an operational plan. Having specific behaviors to do instead of only resisting negative behaviors is critical.
The plan should include several options set up in sequence. The individual or partners try the first behavior. If the first action or activity is not sufficient in of itself to stop the use or behavior or reduce craving, then the individual or partners should go to the next behavior on the list of the plan. As long as the individual or couple works through the plan's list of behaviors, similar to the three actions for dealing with cravings set out by twelve-step programs, the addict is not acting out or using and/or the co-addict is not enabling the addict. Delaying or somehow interrupting the linkage between craving and use or behavior increases the possibility of limiting or stopping addictive behavior. In addition to coming up a plan with specific concrete behaviors, each person and the couple need to identify his or her or their patterns for messing up. People generally are quite familiar with how they mess up… they've done it so many times! "I get kind of tired… then I lose contact with or don't keep up with friends or positive people… or, I get lonely… I don't talk to my partner…" As each partner individually and the couple jointly identifies their patterns, the therapist can help them can make an assessment for clearer predictions of self-sabotage vulnerability. How vulnerable is each partner and are the two of them jointly as a couple to sabotage oneself or the couple's dynamics? Each partner needs to be able to acknowledge how he or she eventually self-sabotages abstinence, personal well-being, or the relationship. In other words, the therapist helps each partner identify personal and the joint self-sabotage patterns. The therapist asks, "How have you messed up before? How will you mess it… yourself, the relationship up again!?" Since negative patterns of use or behavior are inevitably compulsive there are compelling triggers that lead to the individual messing up. In addition, there is some benefit for the individual or couple in problematic or addictive behaviors however distorted or convoluted. So the therapist asks, "Why did you mess up? What was so compelling? What did you get for messing up?"
PLAN II – PLANNING TO AVOID SELF-SABOTAGE
The therapist works with each person and the couple to develop plans to avoid self-sabotage. Most people plan only for success, despite numerous experiences of failure. Planning for their plans to work, they are paralyzed when plans do not work out. Or, they find that they sabotage themselves… again. The therapist should help the partners work out a specific plan for every and any point of vulnerability. Vulnerability may develop for example, when that negative person starts to sound logical, when that toxic person somehow starts to become attractive, or when the individual starts to feel self-pity, or feeling hopeless, or scared. Since the individual or couple tends not to engage in therapy for isolated issues, but for negative or dangerous patterns of behaviors, they should be able to identify their vulnerabilities that lead to acting out or relapse. The individual or couple that claims not be able to identify vulnerability and self-sabotage patterns, usually blames prior negative outcomes on bad luck from circumstances beyond individual or the couple's control. The helpless stance of being victimized by unpredictable world events or uncontrollable outside forces is itself a significant vulnerability that predicts acting out or relapse. The therapist helps the partners work out another plan of action with five to eight behaviors to be tried in sequence. They should work out exactly what each person and the couple are going to do to prevent messing up again. This cannot be a plan to just try harder! Who are they going to call? Who is this partner going to call? The other partner? What are each partner and the couple going to do first? second? third? How do each partner and does the couple going to get help or support? How would each person self-nurture? How will each person and the couple answer those negative thoughts? react behaviorally to negative thoughts?
Since the individual, the partner, and the couple in all probability have a long history of lousy planning and/or failing to follow-through on well-intended plans, the therapist should anticipate high likelihood of failure. The therapist needs to check regularly for both positive outcomes and negative outcomes. If the individual or the couple has a positive outcome, then the therapist must determine if it is a result of applications from their therapeutic planning. A positive outcome may well have resulted from some unanticipated circumstances, choices, and behaviors. Any positive outcome must be examined to determine how and why it happened. Positive outcomes need to be examined so that any identifiable beneficial influences can be maintained for further growth. Positive outcomes are not accidents, nor are they about luck. What was done or wasn't done, what happened instead that made a difference? Whatever one person or the other did well, correctly, "right", or differently made the difference. Give credit to an individual and to the couple. Each person needs to appreciate his or her productive choices and the couple needs to appreciate any improvement. And everyone needs to take note so that he or she can draw back upon the same stuff: resources, skills, and principles the next time. Why? Because there will be a next time! Many next times!
If there is a negative outcome despite planning, the therapist needs to prevent the partners from beating up on each other and themselves. Shaming and finding fault in self or the other partner is one of the negative patterns that need to be broken. Feeling ashamed or guilty, or resentful from being blamed can lead to further destructive communications and actions directed at each other. Or, the addict may engage in self-destructive behavior such as isolating, drinking, denial, and so forth. These are often additional negative patterns to deal with. The therapist needs to guide examination in why and how the negative outcome happened so it can be turned into a therapeutic relapse. A lapse to or repetition of old negative behavior becomes a learning/teaching experience to understand and identify more clearly a person or couple's negative patterns and processes. Examination fosters greater understanding about how addictive use or behavior is triggered and perpetuated. Further clarity is gained about how the use or behavior affects the addict and the partners. The therapist directs attention to each person's emotional and cognitive process and their interactional dynamic. The therapist focuses on uncovering reasons as opposed to making excuses for choices and behaviors. It is important to help the partners avoid self-recriminations and mutual condemnations. Through the discovery process, the therapist helps the partners figure out how to benefit from the experience of failure. The partners will find that each person's process is more complicated than just knowing to "stop it." Normally, the negative outcome resulted not because the new plans were ineffective per se. Failure was usually because one person or both partners reverted to their old patterns of behavior. The therapist's prediction of failure made earlier became realized… again, because one person or both basically did the same negative things, self-sabotaged, and/or sabotaged the other person or process. The therapist needs to challenge each partner and the couple to ask, "What did I learn? What do I individually and as a couple need to be aware of next time? And, plan what do I need to do differently next time?"
PLAN III – RECYCLE PLANS I & II
It often took years to develop the individual or couple's negative patterns and negative processes. The therapist must accept that the individual and couple will take significant time to successfully develop, problem-solve, and sustain positive patterns and positive processes. The therapist needs to remind the partners that frustrating uneven progress is almost inevitable no matter how much either member of the couple wants change and growth to be quick and easy. Therefore, the therapist needs to keep the partners working on repeating and adapting their process over and over. The partners need to go through a second round of further identifying individual and couple's patterns and processes. With their experience, including their failures the partners should be able to recognize more nuances, complications, and exceptions in personal and mutual patterns and processes. The therapist can prompt the partners to make more precise predictions about how each person and the couple will sabotage otherwise logical or effective plans. The Ghost of Xmas Future or the Ghost of Couple's Future returns with another round of more finely tuned prophecies. With therapist assistance, the partners develop a more layered plan with contingencies based on previous complications and failed plans. Essentially, the original plan is taken to a higher level.
The individual or a couple often go through a plan or two, get frustrated, get discouraged and then give up. The therapist should anticipate this as another part of the negative pattern. Sometimes, the individual or the couple actually have effective and productive behaviors in their repertoire and would be otherwise successful. They however fail to follow through on such behaviors consistently. Stopping or quitting from frustration rather than seeking or needing some new behaviors or strategies may be the key barrier to positive growth. Therapy needs to be structured for the individual and the couple to keep on working at the process over and over. The therapist rather than promising a simple quick solution should prepare the individual and the couple to continually examine and adjust their process and plan. Getting the input of the therapist as a professional guide is itself an attempt to break the individual or the couple's pattern or change the process. The therapist needs to be vigilant not to replicate the dysfunctional frustration process by implying a simple quick process. Therapy has to be framed as facilitating an essential trial and error process for the individual and process. The partners need to be reminded that they will go through a lot of frustration and be prepared to tolerate it.
Stopping or quitting precludes the possibility of growth and change. This is true in all therapy or transformative processes, but is particularly vital to assert to the individual or couple that has addiction issues. The addiction is the individual's habitual blocking or blurring of his or her emotional distress from frustration. Repressing or denying negative feeling or thoughts out of consciousness quells motivation for continuing to try to change or grow. It allows the individual to avoid or divert him or herself effectively allowing stopping or quitting with some plausible deniability. Treatment for growth and change for addiction thus, requires addressing eventual and almost inevitable further addictive behavior as intrinsic to the self-sabotaging pattern. Relapse prevention therefore includes expectation and planning for intervention not to work. Therapy has to incorporate the reality of failing and re-using or re-indulging into relapse prevention. The therapist should not act surprised or express disappointment when the individual or couple relapses with substance use or behavioral indulgence. The relapse becomes potentially therapeutic if the therapist uses it to confirm addictive compulsivity and resistance against change of use or behavior. The therapist leads the individual and the couple to dissect how and why the relapse occurred. The transgressing individual often will offer simplistic defensive or condemning excuses for the lapse. This is a victim stance, however aggressively it may be proffered. The addict often asserts that the other partner triggered the relapse through behavior or words, and he or she is the innocent victim/reactor. On the other hand, the relapser may be self-condemning and shameful. In either case, there is a lack of responsibility asserted.
