5. Not Getting It i=In the Couple- II - RonaldMah
Ronald Mah, M.A., Ph.D.
Licensed Marriage & Family Therapist,
Consultant/Trainer/Author
Main menu:
5. Not Getting It i=In the Couple- II
Therapist Resources > Therapy Books > Odd Off Different-Cpl
Off, Odd, Different… Special? Learning Disabilities, ADHD, Aspergers Syndrome, and Giftedness in Couples and Couple Therapy
Chapter 5: NOT GETTING IT IN THE COUPLE- Part II

In addition to the ten reasons for missing social cues discussed in Chapter 4, the therapist should be aware of three additional reasons that can have extremely powerful impact on the couple's relationship. Each of these three reasons: learning disabilities, Attention Deficit Disorder (ADD) or Attention Deficit Hyperactivity Disorder (ADHD), and Aspergers Syndrome are more commonly recognized as potentially relevant to working with children. Appropriate attention and successful intervention to support individuals- children, teens, or adults dealing with these issues also tend to increase intellectual, emotional/psychological, spiritual, and social functionality. Conversely, the lack of attention and poor or absent intervention would cause and predict dysfunction. The therapist may find exploration of these issues in adult individuals may prove relevant to couples dynamics and direct therapeutic strategies. For a particular individual, one or more of these issues may be highly relevant to the couple's core dysfunction.
LEARNING DISABILITIES – Compensation
What Gus says:
"First, find the instructions. Second, get the tools from the garage. Third, open the instructions to page 3. Then, check to see if you have all the components listed on page 3. After that, check with me which features I want to use. Last, figure out exactly where you want to put it."
What Bruce hears:
"First, find the instructions. Second tick tick tick (from the clock)... the garage. Third, open the instructions to page…tick tick. Then, check… (what's that in the yard?) components listed on page 3. After that, gurgle gurgle (water sounds from the bathroom)… to use. Last, rustle rustle (sounds of instruction booklet pages being turned)… tick tick tick… put it."
Anxiety, overwhelm, neuroses, disassociation, and other issues complicating deciphering social cues may arise from individual's struggles with learning disabilities. When other important people's learning and communication styles mismatch with the learning styles of individuals (especially as children) or don't compensate for learning disabilities, then potential increases not just for difficulty in learning and communication but in social interactions or relationships. Peers or partners frustrated or offended by an individual's failure to understand and respond appropriately, label him or her "rude," "mean," and/or "weird." In the example above, Bruce's auditory listening disability draws attention to background sounds (clock ticking, paper rustling, other background noises, etc.) rather than on the "foreground" sounds of Gus' voice. Missing or misunderstanding instructions leads to numerous problems: doing the project incorrectly, acting out to hide ignorance, being perceived negatively, and so forth.
PROCESSING DIFFICULTIES & DIFFERENCES
Individuals with learning disabilities or learning disorders, or who are considered learning different process, integrate, and retrieve information differently, and/or have weaknesses in their processing, integration, and retrieval mechanisms. Learning disabilities are not grown out of, nor do they go away. The educational technical definition for a learning disability is when a child's academic achievement off track from what is expected for someone his/her age. Learning disabilities include deficits in visual perception, linguistic processes, auditory processes, attention, and memory. Examples of learning disabilities and how they can affect recognizing social cues include:
A person who clearly hears instructions but is inefficient in processing the information into short term memory. He or she then "forgets," and gets in trouble. In reality, this is the result of an auditory processing problem;A person who is not as efficient as others in retrieving information from his/her cognitive storage, and thus, takes more time to find the answer to a question. The concentration required to shift through cognitive storage can cause one to become oblivious to other continuing cues. Unaware that the other person has moved on and has asked a new question because he/she had been concentrating on finding the answer, the person with this learning disability gives out that answer for the previous question. His/her correct answer (to the previous question) but incorrect answer (to the current question!) is seen as him/her being funny the first few times, but becomes annoying over time.A person is attentive and understands the information presented, and interacts or responds appropriately verbally, then doesn't follow through very well when required to write something about the information received. The written information come out as disconnected thoughts. Criticized for not trying, the person actually has a learning disability that makes it difficult and confusing as he/she tries to put ideas and opinions in written form.A person is a very slow reader and has always struggled with reading. He/she is thought to not care and/or mentally deficient in school. The person may have an undiagnosed visual perception learning disability creating difficulty in distinguishing the differences in letters that are "mirrors" of each other: "b" & "d", "p" & "q", "M" & "W", "Z" & "N". Dyslexic individuals can become preoccupied struggling to recognize letters and consequently miss or misinterpret social cues.
Distracted trying to compensate for learning disabilities, affected individual may misses emphases from non-verbal facial, tonal, or body language cues. Other learning disabilities can also complicate reading or interpreting social cues correctly. A list of common partner complaints can easily arise out of missing cues because of some learning disability. If identified, individuals can be taught compensations for learning disabilities: auditory challenges with visual compensations; visual difficulties through auditory strengths; and so forth. For example, Bruce can learn to keep his eyes directed at Gus as he speaks. He can rehearse part one of his instructions, part two, and part three not just in his head but out loud verbally. Gus can improve Bruce's integration of his words by having Bruce repeat each part of the instructions as he gives them, before speaking a next part. Giving Bruce time and prompting rehearsal verbally makes it easier for him than trying to recall everything if she spouts all three parts at once. Holding eye contact with Bruce and especially, touching him on the arm when speaking also improves his remembering Gus' instructions. Even better, rather than being frustrated at the likelihood of Bruce forgetting the verbal instructions, Gus can write it all down in a list he can keep and read over multiple times if needed. Bruce can ask for a list, or write down Gus' instructions and make his own list. Bruce also had another undiagnosed learning disability that required additional directed compensations. This did not turn up until later in therapy when Gus and the therapist encountered unanticipated and seemingly illogic resistance from Bruce.
Learning disabilities include a variety of disorders that cause significant challenges in acquiring and using listening, speaking, reading, writing, reasoning, or mathematical skills or abilities. Such disorders are considered intrinsic to the individual. Gus' complaint that Bruce forgets such instructions all the time means that the learning disability is Bruce's for keeps. Bruce could likewise complain that Gus keeps expecting him to be able to transcend his wiring despite clear evidence that is not possible. Learning disabilities are lifelong conditions assumed to be from some central nervous system issue. Individuals may have problems regulating behavior, with social perception, and social interactions, but these are often consequential to learning disabilities rather than themselves being learning disabilities. Identification, ownership, and learned compensations for Bruce's learning disability mitigated further relational distress for the couple. Definitions of learning disabilities recognize that social and emotional problems are important characteristics of the conditions. "However, the current federal definition fails to consider the social-emotional deficits of children and adolescents with LD. Instead the federal definition, which has had an overarching influence on policy and practice, focuses exclusively on academic deficiencies… (Elksnin and Elksnin, 2004, page 4). If recognized in adults at all, the effect of learning disabilities social-emotionally are also often overlooked.
Compared to other individuals without learning disabilities, children with learning disabilities report higher degrees of loneliness and lower levels of peer acceptance. They are more likely to be rejected by peers due to behavior issues and lack of social competency. Disliked or less liked individuals may be put into "four categories: aggressive behavior (destructive tendencies, physical attacks, verbal or emotional offenses, etc.), personality traits (depressiveness, anxiety etc.,), lack of social competence (e.g., in communication skills, problem-solving abilities, social responsibilities, positive attitude toward social activities, etc.), and poor academic and cognitive competence. The most frequently listed reason was aggressive behaviors while poor academic or cognitive competence was the reason mentioned least frequently" (Yu et al., 2005 page 329). Other rejected children show similar characteristics of poor adjustment, anxiety, aggressiveness, and the tendency to violate rules and juvenile delinquency. Isolated and rejected, they are more often lonely. They have fewer positive peer relationships to provide social support and a sense of security. Greater sensitivity and poor self-esteem can contribute to loneliness. With poor social skills for dealing with being lonely, their experience with loneliness may be more intense than that of other children. Poor behavior and social skills rather than poor academic or cognitive abilities are more likely the cause of peer issues and loneliness. Yu et al. assertion that children with learning disabilities need support in schools for their social and behavioral deficiencies (page 330) reminds the therapist that individuals without such support may carry deficiencies into adult relationships. The therapist can readily see how childhood problems caused by learning disabilities can become adult problems in intimate couple dynamics.
"Learning disabled children's lack of social skills (Bruininks, 1978; Bryan, 1974) may be related to difficulty in correctly perceiving moods and intentions of others. Wiig and Semel (1976) suggested that these youngsters encounter frustrations as a result of social misperceptions which may lead to expectations and ultimately initiations of aggression, or may lead to isolation… the learning disabled children appeared to give greater weight to larger movements of body and arms when judging these vignettes… Wiig and Harris (1974) found that learning disabled teenagers also proved less able to differentiate pantomimes of emotions than normal teenagers. However, it is uncertain whether the results of the above studies were due to differences in actual ability to interpret nonverbal cues or whether learning disabled children, especially if they had attentional deficits, were less able to form impressions when dealing with briefly presented stimuli" (Weiss, 1984, page 612). Individuals with learning disabilities interpreted scenes with ambiguous active play more negatively than those without learning disabilities. With quickly shifting social interactions, children with learning disabilities may focus on more easily observed motion cues. In one study, "The addition of verbal cues did not clarify the action presented on the videotapes for the learning disabled boys … although short-term memory was adequate, receptive language and/or language processing deficits might create difficulties in social situations…" (Weiss, 1984, page 614). It is not clear what may be the reasons for these deficits. There are many hypotheses including some which are complementary while others may be contradictory. They include:
"Poor language and communication skills (Bryan, Donahue, Pearl, & Sturm, 1981; Donahue & Bryan, 1983; Mathinos, 1991; Vallance, Cummings, & Humphries, 1998)Difficulty recognizing and understanding others' emotions (Stone & LaGreca, 1983; Wiig & Harris, 1974)Cognitive processing and social-emotional problem-solving difficulties (Conte & Andrews, 1993; Hartas & Donahue, 1887; Tur-Kaspa & Bryan, 1995)Central nervous dysfunction (Denckla, 1986; Little, 1993; Rourke, d1987; Vogel & Fornss, 1992)Comorbid psychiatric disorders such as ADHD, depression, dysthymia (Forness, Kavale, San Miguel, & Bauman, 1998; San Miguel, Forness, & Kavale, 1996)Academic problems and educational isolation that produce social-emotional problems as a side effect (LaGreca & Stone, 1990; Siperstein & Bav, 1988M)History of repeated failure and low self-esteem (Vogel & Forness, 1992)" (Elksnin and Elksnin, 2004, page 3).
While most research and literature has focused on children with learning disabilities, the findings logically predict later successful consequences and problematic dynamics as adults. When adults with learning disabilities were surveyed, "Most reported late development of romantic relationships compared with their nondisabled peers. Finally, participants mentioned difficulties in personal or marital relationships as a result of dependence and/or lack of reciprocity. They frequently needed assistance with certain tasks, which tended to disrupt power relations" (Goldberg et al., 2003, page 232).
MISDIAGNOSED & MISUNDERSTOOD- TRYING HARD BUT "JUST STUPID"
Many individuals- Bruce for example, reach adulthood without identification and remediation of learning disabilities. They may suffer negative consequences but have no theoretical explanation of their difficulties. Other people including parents and teachers may not have noticed and/or individuals may have successfully hidden their learning problems to their personal detriment. The therapist needs to have a general knowledge of learning disabilities and how they impact individual intellectual, emotional, psychological, and therefore, social development. The therapist should explore partner criticisms based on the assumption of full attention, adequate comprehension, solid investment, and clearly implied desired responses of an individual who still makes inappropriate or inadequate responses. The assumption that leads directly to disappointment or a sense of betrayal may need to be qualified if learning disabilities are determined to interfere with full attention and adequate comprehension of messages received. Until Bruce's learning disability was identified, Bruce felt a lot of shame for repeatedly disappointing Gus, and Gus was often hurt thinking that Bruce just did not respect him enough to respond to him as he needed. Individuals with learning disabilities, especially as children are often misdiagnosed. Bruce, like many other children with learning disabilities was seen as mentally deficient, or resistant to learning. Such children are often criticized for not paying attention and being lazy. Off, odd, different, or special may be among the more benign labels they get. They are constantly being told to try harder. Their motivation is questioned. Others including teachers and parents and later, work peers and supervisors and of course, intimate partners often think they don't care. The lack of learning or progress is sometimes seen as the child or employee being defiant or malingering. They may be unaware of their unpopularity. They tend to be less accurate in the assessment of their own social status. They may not be as socially astute to others behaviors or as sensitive to the feelings expressed by peers (Soenksen et al, 1981, page 283). Having encountering failure after failure despite tremendous effort, being constantly criticized and harangued, feeling tremendous frustration, and having had his/her self-esteem devastated, an individual with learning disabilities may start acting out. Subsequently, he or she may fulfill the negative criticisms of being a lazy, unmotivated, stupid, and defiant child. These behaviors can predict similar behaviors as an adult. Early academic failures often predict vocational obstacles and frustrations. The misdiagnosis and being misunderstood continues in adulthood and possibly most problematically in an intimate relationship with a partner.
As children, individuals with 1earning disabilities are constantly being encouraged and admonished to try harder, and constantly being doubted that they are trying hard. Just about all children try very hard to please their parents and to be accepted by other children. So, they try very hard... and then try even harder...and harder. They try as hard as they can, but their learning disabilities may prevent them from being successful; and prevent them from satisfying or pleasing important adults and being labeled negatively. As they try and fail, try harder and fail, try as hard as they can and still fail, they are often stigmatized by adults and other children as being stupid. Worse of all, they believe themselves to be stupid. After all, all that trying just proved it. Individuals with learning disabilities often carry demoralization and diminished self-esteem into adulthood. Loss of self-esteem, as in all individuals makes them vulnerable to a tremendous number of other negative behaviors (emotional problems, relationship problems, violence, defiance, substance abuse, and so forth). Someone such as Bruce was susceptible to all kinds of problematic emotional distress from the damage he endured as an undiagnosed child.
DEVELOPMENTAL INDICATORS OF LEARNING DISABILITIES
Developed by the Coordinated Campaign for Learning Disabilities, the following checklist of characteristics may point to a learning disability. Several of these characteristics (not just one) over an extended period, suggest a possible learning disability. The therapist can explore the history of individuals during key developmental eras to look for early indicators of learning disabilities. Having a child with learning disabilities or difficulties in school may also be an indicator of learning disability in an adult parent, since learning disabilities tend to have genetic concordance.
Preschool
Speaks later than most childrenPronunciation problemsSlow vocabulary growth, often unable to find the right wordDifficulty rhyming wordsTrouble learning numbers, alphabet, days of the week, colors, shapesExtremely restless and easily distractedTrouble interacting with peersDifficulty following directions or routinesFine motor skills slow to develop
Grades K-4
Slow to learn the connection between letters and soundsConfuses basic words (run, eat, want)Makes consistent reading and spelling errors including letter reversals (b/d), inversions (m/w), transpositions (felt/left), and substitutions (house/home)Transposes number sequences and confuses arithmetic signs (+, -, x, /, =)Slow to remember factsSlow to learn new skills, relies heavily on memorizationImpulsive, difficulty planningUnstable pencil gripTrouble learning about timePoor coordination, unaware of physical surroundings, prone to accidents
Grades 5-8
Reverses letter sequences (soiled/solid, left/felt)Slow to learn prefixes, suffixes, root words, and other spelling strategiesAvoids reading aloudTrouble with word problemsDifficulty with handwritingAwkward, fist-like, or tight pencil gripAvoids writing assignmentsSlow or poor recall of factsDifficulty making friendsTrouble understanding body language and facial expressionsHigh School Students and AdultsContinues to spell incorrectly, frequently spells the same word differently in a single piece of writingAvoids reading and writing tasksTrouble summarizingTrouble with open-ended questions on testsWeak memory skillsDifficulty adjusting to new settingsWorks slowlyPoor grasp of abstract conceptsEither pays too little attention to details or focuses on them too muchMisreads information (LD Online).
An individual may appear to have more than one learning disability, have ADHD as well, or have a non-verbal learning disability (NLD or NVLD) that is difficult to distinguish from Aspergers Syndrome. Verbal learning disabilities are often more readily identified, while NLD and Aspergers Syndrome are not as readily recognized, much less distinguished from each other. "There is clearly a great deal of overlap between Asperger's Disorder (AD) and Nonverbal Learning Disabilities (NVLD) – so much so that it is possible that the symptoms of each diagnosis describe the same group of children from different perspectives, AD from either a psychiatric/behavioral perspective, and NVLD from a neuropsychological perspective" (Dinklage, 2008). NLD is considered to be a neurological syndrome characterized by the impairment of nonverbal or performance-based information controlled by the right hemisphere of the brain. "The NLD syndrome reveals itself in impaired abilities to organize the visual-spatial field, adapt to new or novel situations, and/or accurately read nonverbal signals and cues. It appears to be the reverse syndrome of dyslexia. Although academic progress is made, such a student will have difficulty 'producing' in situations where speed and adaptability are required. Whereas language-based learning disorders have been shown to be genetic in origin, heredity has not, as yet, been linked to NLD. It is known that nonverbal learning disabilities involve the performance processes (generally thought of neurologically as originating in the right cerebral hemisphere of the brain, which specializes in nonverbal processing)… Brain scans of individuals with NLD often confirm mild abnormalities of the right cerebral hemisphere" (Thompson, 2008).
NLD individuals often have significant problems interpreting social cues as is also experienced by those with Aspergers Syndrome. Severity of problems reading social cues and interacting socially is thought to be greater and more pervasive with Aspergers Syndrome. NLD children have similar difficulties as children with Aspergers Syndrome in large peer group situations being confused with multiple and complex sets of competing cues. However, they tend to be more adept in one-on-one interactions with adults. Children with Aspergers Syndrome are more likely than NLD children to have other autistic spectrum characteristics: atypical social interactions, repetitious behaviors, or restricted interests (Stein, et al, 2004). One should be aware that professional perspectives (therapist, teacher, social service), including unconscious bias may cause over-diagnosis of learning disabilities and ADHD for minority children. Harry and Klinger's (2007) three-year study on the special education placement process for black and Hispanic students in a large urban school district in a southeastern U.S. state found a disproportionate placement of blacks and Hispanics with a learning disability label. This reverses an earlier historical trend of the diagnosis being given to mainly white and middle-class students. Diagnosis is intended to activate support, however as misdiagnosis it has the opposite effect of causing exclusion from services or maltreatment with inappropriate services. There are many potential social economic status (SES) explanations for the diagnostic differences: prejudice, economic status, educational status, family composition, and so forth that need to taken into consideration to prevent diagnosis becoming harmful. The overlap of diagnoses and potential stereotyping or unconscious bias give caution to the therapist, but should not discourage him or her to assess for potential issues.
COMPENSATION- TRY DIFFERENTLY, NOT TRY HARDER!
The key to successfully helping an individual with a learning disability progress comes from first, recognizing that the individual's lack of success or progress is or is not also due to other issues (especially negatively judgmental issues). Second, the specific learning disability or learning difference needs to be successfully identified. Finally, the therapist needs to help the individual develop compensatory techniques and/or skills. This type of instruction may be specialized. Drawing assistance from and using specially educated and trained professional resources is sometimes required and recommended. Left to their own resources, children may grow into adults with continued problems and/or problematic compensations. There is philosophy in some educational programs to put children with learning disabilities in a less demanding academic environments, give them easier work, and allow them to "succeed" in that way. As a result, some individuals complete public school, get a diploma, and are sent into advanced academic programs and/or the work world as adults without any acquired compensatory skills or techniques. They are unable to function successfully in the real world. And, then they fail, including failing in the intimate partner relationship of a couple. The therapist may need to strongly encourage the individual to learn survival skills or compensations and not just be accommodated or tolerated. The therapist should also challenge the partner who tolerates dysfunctional compensations or accommodations that perpetuate avoidance of dealing with the affected person's challenges.
Individuals with learning disabilities may need work on receptive language and/or language processing skills to improve relationship communication. While the therapist needs to determine if it is within his or her scope of practice or competency, such work may help vocational functioning as well. Individuals may benefit from learning how to select which cues to focus on, especially non-verbal cues. Exercises including role-plays, guided discussion, and storytelling in therapy may improve non-verbal skills and empathy. For example, the therapist might remind or prompt the partner to direct an individual to look at facial expressions before making judgments or taking actions. Rather than focus on aggressive behavior, individuals with learning disabilities may benefit more by using external controls, behavior modification, and/or self-talk that aids self-control. The couple can work on ways to slow impulsive behavior. Therapy can build positive affirmations and methods to counter negative self-esteem from historical poor choices and behaviors. These recommendations for therapy duplicate recommendations by Weiss (1984, page 615) for helping children with learning disabilities.
Successful individuals are able to find vocations or activities that take advantage of strengths rather than those that exacerbate challenges turning them into frustrating failure. Unsuccessful individuals have a greater tendency to avoid trying things that are made more difficult by their learning disability. They had difficulty seeing how their challenges can be compensated for or in identifying alternatives. They may be passive by becoming indecisive or get stuck with ineffectual rigid processes. Such individuals may project the cause of their repeated failures onto others, and subsequently quit trying (page 227). In contrast, more successful individuals remained active and judicious in their activities. They had a greater sense of power and control in how their lives played out. While both unsuccessful and successful individuals could be persistent, successful individuals kept trying but also learned from experience and tried different tactics if the original actions were unsuccessful. Bruce was successful as a craftsman who designed and installed custom cabinet work in designer home. He excelled at the artistic and physical aspects of the work, as well as being gregarious and charming with clients. The paperwork and organization inherent in the work was much harder for him. However, with great determination and sufficient use of resources- both human and technical, Bruce had grown a successful small business. Gus was a major resource and compensated for Bruce in many areas that were challenging to him. Bruce's uncle was a mentor to him both in business and personally. They were very similar- Bruce's uncle in all probability had a similar learning disability.
Of significance in work by Goldberg et al was that "All study participants spontaneously referred to the assistance they had received from others over the course of their lives. They frequently spoke about the support, guidance, and encouragement provided by 'significant others,' such as friends, teachers, therapists, co-workers, and family members" (page 228). "…successful informants demonstrated an enhanced self-awareness and the ability to compartmentalize their learning disability that allowed them to acknowledge strengths as well as weaknesses. They were engaged in the world financially as well as socially, often rising to leadership roles in the family, at work, and in the community. They were decisive, often consulting others for information or advice, and they took responsibility for outcomes. They showed persistence in their pursuits, yet they could be flexible in altering the path by which they skirted obstacles. Successful informants set realistic goals for themselves and demonstrated an awareness of the steps that would be required for their attainment. They made use of the social support available to them in reaching these goals and sought help when needed. In adulthood, they demonstrated the ability to reciprocate and provide care and support for others. Finally, they had developed strategies for recognizing and reducing stress in their lives. Many had developed strong and intimate peer and family relationships that assisted them in many ways to cope with stressful times and maintain emotional stability" (Goldberg et al., 2003, page 230).
The quality of the therapeutic relationship may be a necessary transitional bridge to a positive partner relationship. Or, a positive supportive partner relationship may facilitate getting the individual with a learning disability into couple therapy. As noted by Goldberg, successful individuals are more likely to consult with others. This may include seeking out a therapist. An individual with an undiagnosed learning disability or a diagnosed learning disability not identified as impacting the couple's relationship may depend on the therapist's ability to establish an empathic, supportive, and respectful relationship with him or her. Prior failures of previous authority figures to identify a relevant learning disability and provide compensatory guidance may have terminally affected those relationships. Rather than another insensitive and ignorant authority figure, the therapist may be able to speak to the individual's experience of learning disabilities. From this feedback and subsequent rapport, the therapist may then challenge the individual to set goals and adapt behavior.
STRENGTHS & WEAKNESSES OF DIFFERENT LEARNING STYLES
Someone with a learning disability may have trouble reading and writing but be very adept at putting things together, and understanding how things go together, or reading plans. The therapist may need to help an individual differentiate a learning disability in one area from other abilities in other areas. By isolating a disability or challenge, an individual can keep it from completely and negatively defining him or herself. "Eventually, successful informants reach a level of recognition of their talents along with an acceptance of their limitations" (Goldberg et al., 2003, page 226). Learning style theories say individuals can have stronger and weaker ways of learning. By identifying the learning style of an individual, therapy or instruction can be directed to that style. As a result, the individual is expected to learn more efficiently and with more depth. Auditory learning, visual learning, and motor-kinesthetic learning are common ways to look for strengths and weaknesses in learning styles. When the therapist's style, which will also be some combination of strengths and weaknesses in auditory, visual, or motor-kinesthetic realms, mismatches with the learning style of clients, then there arises the potential for difficulty in learning, frustration in therapy, therapeutic impasse, and termination of therapy. Individuals labeled as "hyper" or active (perhaps, wild as children) are often motor-kinesthetic learners. They learn by using their senses, especially touching and moving about.
A motor-kinesthetic style is often contrary to the style of a partner (or of the therapist) who may value quiet, still attentiveness in a more visual and/or auditory style. Professionals who passed successfully through American schools and systems with primarily visual-oriented and secondarily, auditory-oriented teaching processes may have similar orientations as a group. Individuals with mismatched learning styles would arguably been more likely to fail academically and therefore, less likely to become the professionals, including teachers and therapists for the next generation of challenged children. This could result in a mismatch between therapeutic style (mostly visual and auditory) and the receptive learning style of the motor kinesthetic client. The individual might then be frustrated by not "getting" the therapeutic instruction. The therapist and other partner is then frustrated by the individual's failure. And as the individual gravitates to his/her motor- kinesthetic style, he/she then often becomes too active and frustrated to continue couple therapy. He/she becomes labeled as "resistant to therapy" and/or "non-compliant" and/or "uninvested." Fortunately, Bruce's therapist recognized his learning style and shifted therapeutic interventions and communication to better fit Bruce. For example, the therapist often used a white board and markers to draw cartoons to illustrate important points for Bruce. Having Bruce draw how small he felt when he displeased Gus was more effective than having Bruce explain it to Gus. The therapist guided Gus to use touch and eye contact to increase the quality of auditory verbal communication for Bruce. Rehearsal of communication and lists and notes were introduced to facilitate communication. Role play and empty chair work from Gestalt therapy complemented insight-oriented feedback.
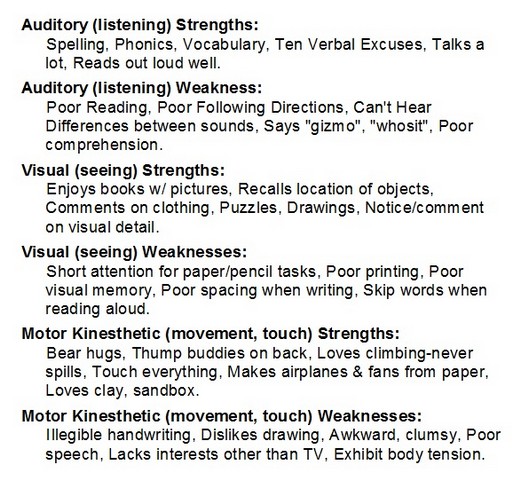
Some individuals have very distinct strengths in one learning style and very distinct weaknesses in the other two. Some individuals, however, are more balanced with relative strength in two or even all three learning styles, with a relative weakness in the remaining style or no weakness at all. In learning situations, individuals can be relatively successful if they have been taught how to compensate for relative weaknesses by using techniques that either draw more heavily on their stronger learning styles, or by using techniques that increase the receptivity of the weaker style. In therapy, the therapist may need to work from either strategy to increase therapeutic effectiveness. For example, a person who is weaker in the auditory style of learning may record a session to listen to again at a pace that he/she can more effectively integrate information. Visual aids, including using a white board to draw and write on during therapy can help a poor auditory learner understand better. A strong motor-kinesthetic learner may benefit from more active therapeutic processes such as role-playing or gestalt empty chair work. Sensory experiences may make certain concepts more tangible to the motor-kinesthetic learner. The following is a summary of strengths and weaknesses using the auditory, visual, and motor-kinesthetic model.
The therapist can explore for these strengths and weaknesses to assess for learning disabilities, along with considering their implications for therapy. These descriptions and other information that expand understanding about learning disabilities help demystify a partner's behavior. Understanding behavior from an identifiable theoretical framework makes it more likely that the non-learning disabled partner become accepting and empathetic. Rather than concluding that less than desired behavior is emblematic of disaffection, disrespect, uncaring, and rejection, the non-learning disabled partner can consider his or her partner's communication and behavior as unfortunately distorted by some learning disability. Goldberg (2003, page 231) said that successful individuals felt they did well because starting in their teens, rather than remediating their learning disabilities, they had "capitalized on a special ability or interest to help them achieve self-sufficiency." As adults, they were able to avoid constantly having to do things that emphasized their weaknesses. They had developed perseverance and used more and varied strategies. They understood that new situations in life with new expectations required that they make adjustments.
The therapist should remain aware that learning disabilities exist among many other important potential influences on the individual and the couple. In a single-risk model, social cognitive and communication problems are considered inherent to learning disabilities that can lead to social relationship problems throughout life, but especially childhood. This can further cause internalized emotional issues such as low self-esteem, anxiety, and depression. Misinterpretation of social cues and difficulty solving social problems can arise out of learning disabilities. On the other hand, a multiple-risk model sees learning disabilities "as occurring in combination with risk factors such as ADHD, poverty, poor parenting, and so forth. This combination predisposes the individual with learning disability to experience social relationship difficulties, which lead to internalizing and externalizing behaviors, which in turn exacerbate risk factors and further fuel relationship problems" (Elksnin and Elksnin, 2004, page 6). While Bruce's learning disability resonated throughout his life and functioning, so did his father's alcoholism, a period of homelessness as a child, peer culture of self-medication with alcohol, and the loss of his dream to be a professional athlete. In addition, while misunderstanding Bruce's learning disability significantly affected Gus' perception of his commitment to him, so did Gus' mix of heteronormative and gay partner role expectations, his childhood with an impoverished borderline single mother, and victimization by bullies for his sexuality in high school. The therapist is challenged and charged to determine what influence and degree of influence learning disabilities may have among other important factors in the individual's and the couple's dynamics.
