4. Intense Emotionality- Bipolar DO - RonaldMah
Ronald Mah, M.A., Ph.D.
Licensed Marriage & Family Therapist,
Consultant/Trainer/Author
Main menu:
4. Intense Emotionality- Bipolar DO
Therapist Resources > Therapy Books > Opening the Can of Worms-Cple
Opening the Can of Worms, Complications in Couples and Couple Therapy
Chapter 4: INTENSE EMOTIONALITY & BIPOLAR DISORDER
by Ronald Mah

Expressed emotion (EE) is a term used to describe a style of family interaction marked by criticism, hostility, and/or emotional overinvolvement. Researchers reported that schizophrenics had higher relapse rates if they had high expressed emotion relatives, than "schizophrenics with low-EE relatives (Brown, Monck, Carstairs, &Wing, 1962). Since then EE has also been shown to have a negative impact of the course of depression (Vaughn & Leff, 1976), alcohol dependence (O'Farrell, Hooley, Fals-Stewart, & Cutter, 1998), and anxiety disorders (Chambless & Steketee, 1999). Family function, more broadly conceived, is also associated with a worse course, and negative treatment outcome, in depression (Miller et al., 1992)" (Gutman, 2006, page 1276). High expressed emotion behaviors develop through a myriad of interactions among life experiences, individual variability, attributional styles, and elements in present relationships. With a couple such as Cole and Molly, there may be no singular causal element to either person's high expressed emotional styles. Intervention and therapy would require a complex diagnosis. "Family interventions should therefore consider
(a) the developmental processes by which high-EE attitudes originated,(b) the ways in which patients process and react to negative affect from parents or other caregivers,(c) the cognitive reactivity of relatives,(d) the ability of patients to manage stressful family interactions, and (e) the behaviors of patients that provoke negativity" (Miklowitz, 2007, page 194).
Emotional reactivity or high expressed emotion often leads to behavior and communication that cooler heads would restrain. Impulsivity or impulsive behavior and communication within the couple's dynamics and in therapy contaminate intimacy and trust. How often does the therapist think, "Oh damn, I wish you hadn't said that!" or listen with dread during the narrative about the toxic choices during the battle of the week? "How couldn't you know that would just make things worse?" The answer is often that the individual does know but impulsively blurts it out anyway, or is so emotionally aroused and triggered that he or she lacks the restraint to pause and consider the ramifications. Impulsivity "does not appear as a separate syndrome in the DSM system, but may be featured as one of several, qualitatively different types of behaviour, which when clustered together, lead to the assignment of a particular diagnosis. The adult psychiatric disorders most associated with impulsive behaviour are mania, substance abuse and the personality disorders" (Evenden, 1999, page 352). By definition to be considered a substance abuse disorder, substance use has become serious, malignant, and resistant to treatment. It "must consist of two components -poor impulse control when it comes to assessing the dangers of the substance abuse, coupled to very good impulse control when it comes to feeding and hiding the abuse" (Evenden, 1999, page 352). Impulsivity is seen basically as qualitatively problematic behavior. While controlling impulsivity is a goal of many treatment protocols, the paradox exists that such a goal means developing volition over what is not volitional. Impulsivity may be better conceptualized for individual and couples dynamics along a continuum of high impulsivity difficult to restrain or alter to low impulsivity readily amenable to restraint or change. While this conceptual shift may help diagnosis and direct intervention to behaviors most available to change, a more productive strategic shift may be to determine what causes impulsivity. With such understanding, then issues may be addressed to give individuals and couples greater choice and control over what had been non-volitional or impulsive previously.
Related to impulsivity is high persistence behaviorally or an inability to give up dysfunctional choices. "Persistence can be defined as the tendency to pursue goal-directed behaviour for a long time in unfavourable circumstances" (Evenden, 1999, page 358). Emotionally reactive partners not only impulsively choose negative behaviors and communications, but also persist with them despite repeated negative consequences. Just "say no or don't do it anymore" or "just stop it" are logical therapeutic interventions that are intellectually considered and accepted as beneficial and effective. However, for some individuals activated in the couple, it just is not possible… or it just is not that simple. Cole and Molly are otherwise intelligent and competent individuals in almost every other realm of their lives. Both partners excel in their work and in the community. They can participate in the therapeutic analysis of how they have made poor choices and what would be better choices next time they engage negatively. And then, make the same bad choices all over again. While they may accuse each other of being so obnoxious and provocative that each was compelled to choose poorly again, they also feel shamed for transgressing while knowing better. Knowledge or communications insight about "good" versus "bad" communication proves insufficient for partners such as Cole and Molly. Rather than assess and label individuals with high to low negative persistence, therapy may better serve functionality by determining what causes them to persist. Rigid thinking that makes alternative options unavailable often causes negative persistence. First-order thinking leaves an individual only considering choices in the first order range of options, while unacknowledged rules and boundaries make effective choices in the second order unavailable. Exploring what are the limiting rules and boundaries may be can free individuals to let go of negative persistence.
For example, Cole impulsively and persistently denies his emotions because of his male rules for affective stoicism. The rule is that he cannot own and express emotions and still be a man. If Molly or the therapist encourages him to express his feelings, he will persist in his reticence. He won't violate his man-rule, despite his resistance being to his detriment. Therapy should address the rule underlying his negative persistence. The therapist can then offer that he can own and express and be still be a man. Manliness is challenged as not just a set of rules, but expressed in some purposeful principles. As he is guided to consider and accept a principle of emotional connectivity and shared expression as a key male trait, then he can be a different and better man that is more supportive of Molly. On her part, Molly is continually disappointed that Cole does not intuit her emotional distress when she presents a problem at work. Despite her disappointment, she persists in silently (and sometimes, not so silently) being resentful rather than saying something. Her rule is that if Cole loves her, he will automatically intuit her emotional distress and immediately nurture her. And, that telling him specifically about her distress and asking for nurturing would make any subsequent nurturing not count. When Cole has asked her to just tell him what she wants, she won't. Therapy can challenge the two rules and assert that his lack of intuition comes not from not caring, but from an emotionally limited model of nurturance. Thus getting what she needs by educating (telling) him still counts and becomes a viable option.
Choice comes out of deeper work and understanding. Impulsivity and negative persistence can lose their rigidity when underlying issues are addressed. Impulsivity and negative persistence both contribute to and are consequences of problematic systemic dynamics. They are reciprocally related to overall stress. In addition, stress in the relational system can be determined by ascertaining whether an individual lives with others with high expressed emotion (EE) attitudes (that is, high emotional reactivity). Individuals with high expressed emotion rate high in expressing criticism and hostility, as well as emotional overinvolvement. Individuals with bipolar disorder have their own issues with expressing and acting out high emotion triggered in the manic phase. Manic emotions and behaviors can elicit intense emotional response from partners and family. Emotional overinvolvement by a parent or partner can occur "…during or immediately following a patient's acute episode of illness… Patients with schizophrenia, bipolar disorder, or recurrent major depressive disorder who return home to high-EE families following an acute episode are two to three times more likely to relapse in the subsequent 9 months than are patients who return to low-EE families (Barrowclough & Hooley, 2003; Miklowitz, 2004)" (Miklowitz, 2007, page 193).
Hyde (2001) referenced Nathan Ackerman promoted family therapy to address individual mental problems. Ackerman identified four ways that families deal with crisis:
1. The family confronts, accurately defines, and achieves a realistic solution of its problems.2. Though unable to achieve a realistic solution, the family can nevertheless contain the problem and control the potentially noxious effects while giving itself a larger period within which to find a solution.3. Unable to find an effective solution or to contain the destructive effects of conflict, the family responds to the tension of failure with an "acting out" pattern of impulsive, ill-judged, self-defeating, harmful behavior. Sometimes the family as a group seeks a scapegoat, whether within the family or outside. In this condition the family as a family system cannot long maintain its defenses.4. With persistent failure at the presiding three levels, the family shows increasing signs of emotional disintegration, which in some circumstances may culminate in disorganization of family ties. (Hyde, 2001, page 111-12).
Individuals such as Cole and Molly often come into their couplehood and the therapy from historical experiences within their mutual families that model and predict their interactional patterns. It is reasonable to presume that individuals from families that deal with crisis (including non-bipolar disorder crises- neither Cole or Molly have bipolar disorder) in the first two ways would tend to have both more skills and confidence during intimate conflicts. On the other hand, it also would follow that individuals who have experienced the high emotion expression (EE) or emotional reactivity of the last two ways of dealing with crisis would become more vulnerable to replicating such reactivity in their intimate conflicts. However, assuming direct causation of high emotion expression from family experiences would ignore the impact of a variety of other factors. A child may have temperamental traits or vulnerabilities such as irritability, low frustration tolerance, mood instability, high anxiety or compromised cognitive functioning. "These early disturbances partially reflect the child's genetic vulnerability to bipolar, schizophrenic, or other psychiatric disorders" (Miklowitz, 2007, page 193). With a sensitivity or vulnerability, a particular child may be matched with a parent "who, by virtue of his or her own neurobiology and social history, reacts to the child's behavior with frustration and hostility." This would be particularly toxic if the child has some significant disorder or challenge. Any issue would be intensified with constant parental criticism that corrupts the child's self-esteem. Or, an anxious or insecure parent may act out issues with smothering and over-protective actions. "Repeated exposure to criticisms, anxiety, or overinvolvement during the period when a child is developing a sense of identity may contribute to self-doubt, self-criticism, and core beliefs about relationships as aversive and conflict-ridden. These schemata for the self may interfere with the child's acquisition of emotional self-regulatory skills, as reflected in depression, anxiety, aggression, and the inability to tolerate negative states of affect. In turn, his or her negative counterreactions fuel high-EE attitudes and behaviors in parents, which recursively contribute to the child's emotional and cognitive vulnerabilities" (Miklowitz, 2007, page 193).
The negative dynamics are further exacerbated by the tendency of high-EE relatives to blame a reactive behavior of the child or partner to personal choice. In other words, although their behavior may trigger the emotionally reactive individual through systemic dynamics, the family member or partners tend not to acknowledge their responsibility. Instead, they attribute the poor choices and emotional reactivity to something that the reactive child or partner can or should control: lack of motivation, poor values, minimal effort, and other personality factors. High emotionally reactive partners or relatives may easily misinterpret a complex and poorly understood issue such as bipolar disorder. On the other hand, low-EE relatives are more likely to attribute the acting out person's behaviors to uncontrollable or difficult to control factors such as illness or external stressors such as work issues. In other words, they are less likely to blame the individual. "Several studies find that high-EE relatives and patients are more likely than low-EE relatives and patients to be engaged in negative cycles of verbal and nonverbal interaction during the postepisode period (for review, see Miklowitz, 2004)" (Miklowitz, 2007, page 193). Cole and Molly experience each other's behavior from current and old lenses. If either partner has a negative attributional perspective, their instinctual reactions would tend not to compassion or a willingness to consider external stressors. The following explanation and graphic from Miklowitz that looks at the systemic dynamics of a person with bipolar disorder can be applied to other issues.
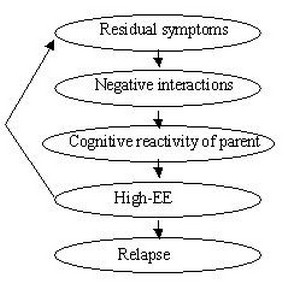
In Fig. 1, "Bidirectional relationship between parental expressed emotion (EE) and patients' mood symptoms. The pathway begins with unresolved residual symptoms in the patient (e.g., depression, irritability, mild delusional thinking, withdrawal, hypomania) that contribute to the intensity of the patient's reactions to caregivers. Escalating negative interactions reduce the threshold for caregivers to react with fear, frustration, and hopelessness; remember and exaggerate negative experiences from prior illness episodes; and make attributions of controllability and negative predictions about the future (e.g., 'She's doing this to hurt me''; 'I'll always have to take care of him'). This 'cognitive reactivity' of the caregiver may fuel his or her expression of high-EE attitudes toward the patient, resulting in temporary exacerbations of the patient's residual symptoms and a worsening pattern of dyadic interaction. In combination with biological and genetic vulnerability factors, repeated exposure to negative family interactions may contribute to the patient's overall liability to early relapse" (Miklowitz, 2007, page 193).
This model can apply to other emotional or behavioral choices that may distress or challenge the couple or family. Residual symptoms in the couple could be adult attachment style from early insecure attachment, mismatched cultural models, prior trauma, anxiety or depression from the family-of-origin or academic or social frustration and failures, and so on. Negative interactions may manifest in individuals such as Cole or Molly when they enter the relationship with hypersensitivity and vulnerability to various triggers along with poor inter-relational skills. The descriptions of Cole and Molly are comparable to cognitive reactivity as partners to each other as opposed to cognitive reactivity as parent to child. Their high EE or emotional reactivity exacerbates their residual symptoms (insecurity, low self-esteem, etc.) and toxic patterns (criticism, defensiveness, stonewalling, etc.). The cycle of residual symptoms that lead successively to more negative interactions, cognitive reactivity, and high-EE cause more acting out- relapse. As the problematic process intensifies and relapse can manifest as explosive intimacy annihilation and violations of the couple's emotional contract.
When the therapist works with a couple, he or she often holds a model of a healthy couple or family. The therapist should be aware if the model assumes low emotional reactivity and high cognitive functioning. Gottman implies a model when he identifies how regulated couples function more positively than non-regulated couples. In a healthy system or couple, there is the greater presence of positive traits and behaviors and the lower presence of negative traits and behaviors. Hyde (2001, page 12) presented a list from the work of Jerry M. Lewis and his colleagues. They identified the following five characteristics of healthy family functioning:
Mutual affection and trust in one another and the communityRespect for individual differences in perception and feelingsThe ability to communicateThe ability to accept lossClear-cut boundaries between parents and children
Hyde proposes an addition characteristic of empathy. Having empathy for a challenged partner can be very difficult. The stress on the non-challenged partner can be extremely distressing and burdensome. The couple has to endure major mood swings with the high emotional reactivity of the challenged partner. Problems consequential to emotional outbursts and volatility can intrude upon the relationship. Emotional reactivity and other stresses cycle repeatedly to intensify problems in all areas. A challenged person may begin to doubt everything and feel out of control. Becoming desperate, he or she may battle against a partner or others who are trying to help. A negative self-image develops or is perpetuated. Every consequence for the challenged person may be duplicated in the other partner. It can become virtually impossible for the other partner to see the challenge, condition, or disorder as he or she becomes depleted dealing with never ending crises. The challenged person's behaviors are interpreted as intentional, disrespectful, selfish, and scary choices. While the other partner's affection and support may be appreciated, they are insufficient in of themselves to alter or curtail problematic feelings and behaviors. Basically, love is not enough. Both the challenged individual and the other partner (and other family members) need a forum, guidance, and support to work through complex emotions from living and dealing with the emotional reactivity and the disorder or issue. Both the challenged individual and family members need opportunities to sort out the complicated feelings associated with behavior, education, medication, personality traits and communication. "Thus, we turn to family therapy and family treatment as mental health resources for the family and the patient" (Hyde, 2001, page 111).
Relational systems where members, including the person with a challenge, "have the ability to express empathy for each other are more capable of adapting and accommodating to the ups and downs of" a challenge than those without empathic members. For example, when Cole was distraught over his father's illness, he emotionally shut down. It looked very bad, and no one knew if his father would make it. Fortunately, Cole's father pulled through. Molly who both felt and expressed her emotions would have been perplexed ordinarily with Cole's reaction. However, she knew that Cole cared deeply for his father despite lacking readily recognizable overt emotional communications and behaviors. She refused to take his stoic demeanor at face value and spent a lot of energy to understand his emotional response and his instinctive, if ineffective coping mechanisms. Molly showed her understanding and support by cueing the children. She explained to their children, "Daddy is sad and worried about grandpa. He gets quiet when he worries. You can help him by giving him a hug." The stress of his father's illness did not intensify the couple's problems. Cole's experience of Molly's empathy allowed him to become more emotionally in touch and reveal more of his inner process
In a contentious situation however or when interactions have taken a negative turn, some individuals get waylaid by emotional reactivity and lose empathy. Once again, the circularity of the solution to the condition and the consequence of high emotional reactivity being the development of low emotional reactivity direct and yet preclude resolution of problems. Mutual affection and trust, respect for differences, communication skills, tolerance for loss, and healthy boundaries get broken down. Empathetic in calmer and non-conflictual interactions, partners sometimes experience feelings as an either-or situation. Connecting with and honoring the other's feelings ends up meaning giving up one's own feelings. This feels unacceptable. This complicates partners from seeing or feeling things from the other's perspective. If challenged partners habitually get stuck in an egocentric view, they cannot recognize the disruption and despair any problematic behaviors may cause to others. As this persists, the couple or family slides towards dissolution. Conversely, empathy facilitates cooperation and win-win problem solving. Couples with low EE are better at recognizing when they get stuck and when partners are mutually harmed. When the therapist can guide and instruct partners towards empathy and lower emotional reactivity, problem solving and intimacy improves.
The therapist tries to create a safe enough therapeutic environment- a good enough therapeutic community for the partners to develop skills and work out problems. Therapy becomes the practice place and model for creating a good enough couple or family for the partners where it has not been particularly good enough or safe enough. "I find it particularly important to establish the therapeutic situation as an area of safety, a holding environment (Winnicott, 1965), that the couple can use as a secure base from which each can explore his or her wishes to be understood by the other (Clulow, 2001). The therapist's ability to accept all of the partners' affects, especially the unexpected, disorganized ones, contributes to this containment and holding. The holding environment is not just part of an overall relationship but is one element in the therapeutic action. It is a change agent in its own right because it provides an ambiance different from what existed in each partner's family of origin and can serve as a model for the emotional tone that the partners might be able to create" (Feld, 2004, page 424-25).
The therapist must be aware of the dynamics within the session among all participants: the therapist and the two partners. As the partners may be prone to intense emotional interchange, the therapist will need to be self-aware and manage his or her own emotions. The couple's high emotional stress and chaotic interactions can challenge not just the safe holding environment of the session, but also the therapist's intrapsychic serenity. The better the therapist is able to self-regulate his or her internal psycho-emotional and intellectual process amidst the session's drama, the better the therapist may be able to respond skillfully for the partners. The therapist's calm involved participation is a model for one partner self-regulating in a healthy manner despite volatile and provocative behavior by the other partner. Unfortunately, dynamics of the couple may be so toxic that far from facilitating an ideal safe haven, the therapist may be drawn into their chaos and become disrupted as well.
